Balancing Safety and Efficiency in Community Pharmacy
Efforts to address the high workload and multifaceted nature of patient care in community pharmacies may lead to prescription processing practices that can put patient safety at risk. This bulletin highlights the findings from a multi-incident analysis of errors reported in the community pharmacy setting and identifies opportunities for process improvements.
INTRODUCTION
Efforts to address the high workload and multifaceted nature of patient care in community pharmacies may lead to prescription processing practices that can put patient safety at risk.1-5 This bulletin highlights the findings from a multi-incident analysis of errors reported in the community pharmacy setting and identifies opportunities for process improvements.
METHODOLOGY
Medication incidents submitted between March 2017 and June 2019 with a setting of “community pharmacy” were extracted from 3 ISMP Canada voluntary reporting databases* (National Incident Data Repository for Community Pharmacies,† Consumer Reporting, and Individual Practitioner Reporting). The search included key terms commonly used to describe problematic practices in the community pharmacy setting, including “circumvent”, “workaround”, “shortcut”, and “copy-over”. Of the 192 incidents identified, 94 were included in the analysis. The analysis was conducted according to the multi-incident analysis methodology outlined in the Canadian Incident Analysis Framework.6
FINDINGS
The analysis identified 6 areas where measures intended to expedite prescription processing contributed to medication incidents. These measures can be grouped within 3 stages of prescription processing in community pharmacies: order entry, filling, and pickup (Figure 1).
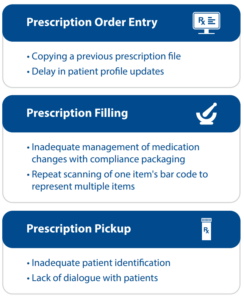
FIGURE 1. Problematic processes grouped by prescription processing stage – order entry, filling, and pickup.
PRESCRIPTION ORDER ENTRY
Prescription intake encompasses receipt of prescriptions from patients or prescribers, as well as entry of prescription information into the pharmacy software system. Order entry is completed by a member of the pharmacy team and the information is verified for accuracy.
Copying a Previous Prescription File
When entering a new prescription into the patient’s electronic profile, an existing prescription for the same medication can be copied, with the intention of changing fields as required to reflect details of the new prescription. During training, employees are often taught how to use the copy function to expedite prescription processing.
Incident Example
A new prescription for methylphenidate 20 mg was entered by copying the patient’s previous prescription record for methylphenidate 10 mg. The pharmacy staff member entering the prescription overlooked changing the strength field from 10 mg to 20 mg, resulting in the patient receiving half the intended dose.
Delay in Patient Profile Updates
When presented with a prescription for a current medication with a different strength or altered directions for use, or for a different drug for the same indication, the pharmacy team may focus on filling the new prescription right away. Workload and time constraints may then delay inactivation of previous prescription(s) in the patient’s profile.7 When discontinued prescriptions remain on the profile (and are displayed as “active”), these can inadvertently be dispensed, resulting in medication errors (i.e., duplicate therapy) and possible patient harm.
Incident Example
A new prescription for a beta-blocker included a note to discontinue the patient’s current beta-blocker. However, the prescription for the beta-blocker on file was not discontinued or inactivated. The prescription for the previous beta-blocker was refilled soon after the new one was dispensed. The concomitant ingestion of both beta-blockers was reported to have contributed to the patient’s death.
PRESCRIPTION FILLING
Prescription filling involves retrieving the medication, preparing the quantity required for the prescription, packaging the medication in a suitable container (e.g., vial, bottle, or compliance package), and labelling the container.
Inadequate Management of Medication Changes with Compliance Packaging
The preparation of compliance packages (or blister packs) is complex, involving multiple steps and, potentially, several pharmacy team members, and is often completed in advance. The analysis identified numerous reports where midcycle changes to a patient’s medication regimen (i.e., before the patient’s next blister pack was due to be prepared) contributed to medication errors.
Incident Example
A patient, who was partway through a blister pack, had the dose of one medication changed from 2 tablets daily to 3 tablets daily. A vial containing tablets of this medication, labelled with the new instructions, was given to the patient, to be taken during the interval until the next blister pack was prepared. The patient misunderstood the instructions, and took 3 tablets daily from the vial, in addition to the 2 tablets in the blister pack, which resulted in a total daily dose of 5 tablets.
Repeat Scanning of One Item’s Bar Code to Represent Multiple Items
Workarounds intended to expedite the filling process bypass the intended safety advantage of bar-code scanning.8,9 An example of a common workaround is scanning the bar code on 1 item multiple times, rather than scanning the bar code on each item separately, when more than 1 package of a medication is needed to fill a single prescription.
Incident Example
When filling a prescription that required 3 boxes of medication, a pharmacy team member scanned the bar code on a single box 3 times, instead of scanning each box separately. The boxes were then taped together, with 1 label affixed to the 3-box package. Fortunately, during the visual product check, the pharmacist identified that 1 of the boxes contained the wrong strength of the medication.
PRESCRIPTION PICKUP
Prescription pickup refers to the act of transferring the filled prescription from the pharmacy to the patient. This last stage of prescription processing offers an opportunity for a final check to detect and prevent any medication errors from reaching the patient.
Inadequate Patient Identification
Pharmacies should follow strict procedures for patient identification at pickup, such as asking for 2 patient identifiers and having the patient and pharmacy staff member double-check the containers in the bag together before leaving the pharmacy.5 Of particular concern for example, inadequate patient identification processes led to several “wrong patient” errors associated with opioid agonist therapy (e.g., methadone, buprenorphine-naloxone).
Incident Example
A patient picking up a prescription confirmed the last name and provided a nickname as their first name. The pharmacy staff did not request a second patient identifier, and as a result, the patient left the pharmacy with another patient’s prescriptions.
Lack of Dialogue with Patients
Patients should receive counselling about all new prescriptions, including those with a change in dose or directions for use. Many pharmacies have systems in place to alert pharmacists to prescriptions that require discussion with the patient; however, factors such as interruptions or high workload may result in these alerts being overlooked.3
Incident Example
A patient who was taking warfarin received new prescriptions for 2 antibiotics that had the potential to increase the effect of the anticoagulant. The pharmacist did not communicate to the patient’s agent (who picked up the prescriptions) the need for more frequent bloodwork monitoring to mitigate the risk of bleeding. The patient was later hospitalized because of severe bleeding.
CONCLUSION
The complex demands of patient care and the often high-pressure practice environment are key considerations when designing workflow in community pharmacies to ensure that processes and systems do not compromise patient safety.2,3,5 Learning from the analysis of these errors is shared to help pharmacy teams better understand the potential risks associated with problematic processes and to encourage consideration of how various technologies and available resources can be better utilized to optimize efficiency and safety.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.