Gaps in Interconnectivity of a Hospital’s Electronic Systems Create Vulnerabilities at Transitions of Care
This bulletin explores a case of a morphine overdose during a transition of care between 2 hospitals. The error was a result of a discrepancy created by an electronic medication system that did not communicate in real time.

- Recognize the need for seamless communication, in real time, among electronic systems housing patient medication data.
- Develop processes to transfer information among stand-alone electronic programs and/or systems.
- Help staff and physicians to recognize gaps in electronic communication that could affect their daily practice and patient safety.
- Consider using the safety tool Hospital to Home: A Medication Safety Checklist for Transitions, including its recommendations for dialogue with the patient and/or family, when preparing patients for discharge.
INTRODUCTION
“Transition of care” is a term describing the movement of patients between healthcare locations, providers, or different levels of care within the same location, as their conditions or care needs change. Fragmentation in the exchange of patient information between sending and receiving practitioners and facilities often makes this a vulnerable time in a patient’s journey through the healthcare system.1 Transitions of care constitute a priority focus of the World Health Organization’s third Global Patient Safety Challenge, entitled Medication without Harm.2 Many acute care hospitals have electronic medication-use systems to facilitate various tasks, including order entry and verification, medication packaging, dispensing, and administration, as well as generation of discharge prescriptions.
In some hospitals, a single integrated system is used to perform all such functions, and there is no need to manually transfer information from one system to another. Other facilities may conduct some tasks using stand-alone electronic systems or may continue to use paper-based methods for certain functions. In the latter 2 scenarios, a human intervention is required to transfer data from one system to another. Even integrated systems may not offer real-time updates (e.g., information in certain fields may be updated only at the time of the daily back-up), which means that outdated medication data will be temporarily available in some parts of the system. This bulletin shares one of several medication incident reports received by ISMP Canada involving an error that resulted from a communication gap between electronic systems within a single organization during a transition of care.
INCIDENT EXAMPLE
A patient who was receiving long-acting morphine 100 mg orally twice daily at home was admitted to an acute care hospital. During the hospital stay, the patient’s pain medication was intentionally changed to fentanyl 25 mcg patch applied topically every 72 hours, which was administered for almost 2 weeks. The day before the patient was discharged to a rehabilitation hospital, the prescriber discontinued the fentanyl and ordered long-acting morphine 100 mg orally twice daily, the same dose taken at home prior to admission. This change was captured in the patient’s medication administration record (MAR), which was then sent to the rehabilitation hospital.
On the day of discharge, another prescriber changed the morphine dose in the stand-alone electronic discharge prescription system. The prescription was written for long-acting morphine 50 mg orally twice daily, as the prescriber thought it better reflected the equianalgesic conversion for the fentanyl dose. In both the discharge prescription and the discharge summary, morphine 50 mg orally twice daily was erroneously documented with the notation “unchanged [from home dose]”.
The pharmacist at the rehabilitation hospital recognized the discrepancy between the morphine dose recorded in the MAR and the dose entered in both the discharge prescription and summary. This pharmacist then checked multiple sources to clarify the morphine dose. A pharmacist at the acute care hospital was contacted and confirmed that the pharmacy system showed that the last dose regimen documented in the MAR was for morphine 100 mg orally twice daily. The community pharmacist and patient were also consulted, and both confirmed that the home dose before admission had been long-acting morphine 100 mg orally twice daily. Based on this information, the healthcare team at the rehabilitation hospital ordered and administered long-acting morphine 100 mg orally twice daily. The patient was found unresponsive at the rehabilitation hospital 2 days after admission and was sent to an acute care hospital for treatment of morphine overdose.
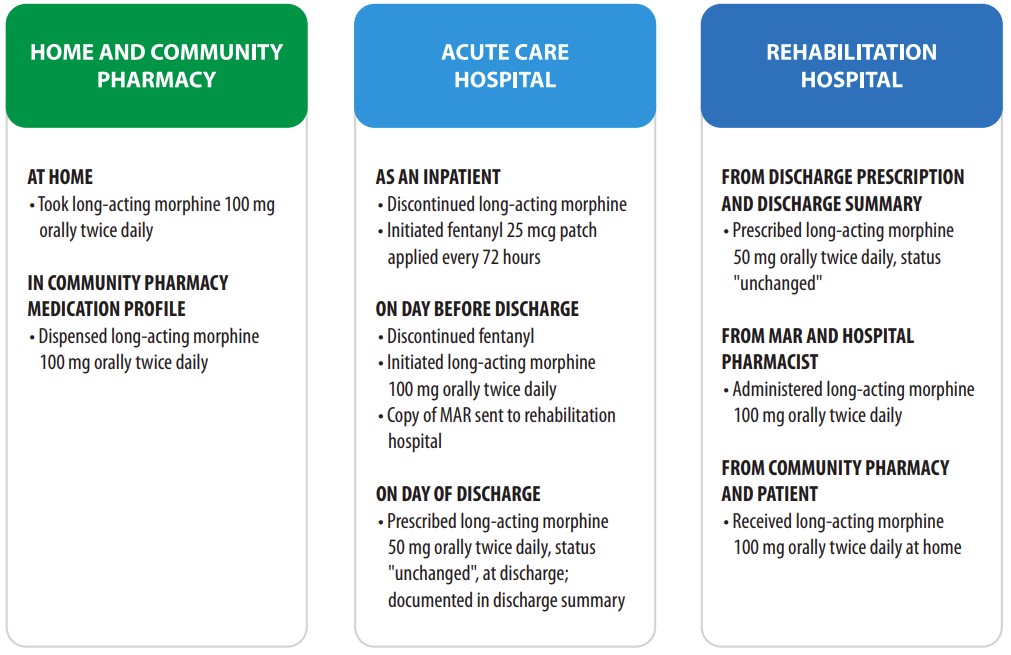
FIGURE 1: List of the patient’s opioid medication regimen at each transition of care. MAR = medication administration record.
DISCUSSION
When a hospital transfers a patient to a rehabilitation hospital or other non-acute facility, it is common practice to send advance information about the patient’s current medications (typically in the form of a copy of the most recent MAR), usually on the day before discharge. The receiving facility then checks the MAR to ensure the medications needed are available to avoid any interruption in therapy.
The general perception at most receiving facilities is that the MAR represents the most up-to-date medication profile for patients who are being transferred and therefore that medications are unlikely to change further. With the MAR being sent on the day before discharge, last-minute changes to the discharge prescriptions and discharge summary may lead to discrepancies. In the incident example described here, staff at the rehabilitation hospital did not realize that the prescriber had intentionally lowered the dose of morphine on the discharge prescription, and the prescriber might not have been aware of the hospital’s procedure of sending a patient’s MAR to the receiving facility on the day before discharge. Automation complacency3 (a strong belief in the accuracy of technological tools) may also have played a role. This factor might have led the prescriber to erroneously believe that information entered in the discharge prescription system would be seamlessly transferred into all the hospital’s electronic systems containing medication-related data fields, such as the MAR and the discharge summary.
Staff at the rehabilitation hospital identified the discrepancy in the morphine dose. Because of this discrepancy and the “unchanged” notation, the pharmacist for the rehabilitation hospital checked 3 additional sources of information, which confirmed that the patient’s morphine dose before admission to hospital had been 100 mg, not 50 mg. Staff at both hospitals were not aware that the system used for preparing discharge prescriptions in the acute care hospital did not communicate electronically with any other electronic systems containing medication data, and that information entered as a discharge prescription would not be captured anywhere else.
RECOMMENDATIONS
Transferring Facilities: Management
- Emphasize to personnel overseeing strategic planning and purchases for information technology that electronic systems housing patient medication data should ideally communicate seamlessly with each other, in real time, to support patient safety.
- Identify existing stand-alone electronic systems to:
- develop processes to transfer information between systems;
- address electronic communication gaps as part of ongoing resource planning for system improvements; and
- help staff and physicians recognize electronic communication gaps that could affect their daily practice and patient safety.
- Design the discharge prescription and discharge summary forms to include contact information for the most responsible physician, the discharging nursing unit, and the hospital pharmacist, to facilitate clarification of medication queries after hospital discharge.
- Allocate time and resources to conduct quality medication reconciliation at transitions of care.
Transferring Facilities: Practitioners
- Report concerns about lack of interconnectivity between electronic systems to department managers and to personnel responsible for facility safety or risk management.
- Consider using the Hospital to Home: A Medication Safety Checklist for Transitions4 (https://www.ismp-canada.org/transitions/) to prepare patients for discharge. The checklist is intended to be used for patients returning home, but many of the recommended activities are also relevant when patients are discharged to another facility. Key elements of the checklist are creating the best possible medication discharge plan, discussing discharge medications with the patient and/or caregiver, and connecting with community partners (e.g., the pharmacist at the receiving facility) to provide updated medication information.4
- Outline the rationale for any medication changes on the discharge prescription. In this case, a statement such as “dose reduced to reflect analgesic needs” would have provided key supplemental information to the receiving facility.
- Engage in dialogue with the patient and/or family about any differences between the medication regimen taken at home before admission, the regimen received while in the hospital, and the regimen to be provided at the receiving facility.
Receiving Facilities
- Conduct admission medication reconciliation in a timely fashion, to identify and clarify ambiguous information. If a discrepancy is identified, communicate directly with the primary prescriber or the pharmacist from the transferring facility, if possible.
- Anticipate that medication or care regimens may be altered by the sending facility at the time of discharge and develop processes to verify that the discharge prescriptions reflect those changes.
- Ask the patient and/or family if they are expecting any changes to the medication regimen received in the hospital.
CONCLUSION
The implementation of electronic medication systems can help to prevent medication errors, but these systems can also contribute to errors when they do not communicate with each other in real time. Last-minute medication changes are often made when patients are discharged from acute care facilities. Therefore, it is important that a hospital has internally linked or integrated systems, that are able to share the most up-to-date information in a timely fashion. Engaging patients and caregivers in a discussion about the discharge medication regimen will further support a smooth and error-free transition of care.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.