Good Catches in Community Pharmacies: A Multi-Incident Analysis
The multi-incident analysis reported here highlights practices and processes that resulted in successful interception of errors in the community pharmacy setting.
INTRODUCTION
Near misses are incidents that could have led to harm but were detected and addressed before reaching the patient.1 Learning from these incidents reveals processes that help in detecting errors and also illuminates opportunities for continuous quality improvement.2 At present, limited Canadian data are available concerning interventions by community pharmacy teams to correct errors before they reach the patient (also known as “good catches”).3,4 The multi-incident analysis reported here highlights practices and processes that resulted in successful interception of errors in the community pharmacy setting.
Near Miss or Good Catch Definition:
An event that could have resulted in unwanted consequences but did not because either by chance or through timely intervention the event did not reach the patient.1
METHODOLOGY
Reports of incidents submitted between April 1 and April 30, 2023, to the National Incident Data Repository for Community Pharmacies (NIDR)* with the outcome “no error or near miss† – circumstances or events that have the capacity to cause harm” were extracted for review. Reports were excluded if the incident described did not conform with the Canadian Medication Incident Reporting and Prevention System’s definition of a near miss.1 The incidents were analyzed according to the methodology outlined in the Canadian Incident Analysis Framework.5
QUANTITATIVE FINDINGS
A total of 1255 incidents were identified and screened for inclusion. Of these, 534 incidents were excluded because they did not meet the definition of a near miss. The remaining 721 incidents were included in the data set for quantitative and qualitative analysis.
Most of the near-miss events (52%) were discovered during prescription verification in the dispensing process (Figure 1). Prescription verification includes both checking the order entry in the pharmacy system against the original prescription and verifying clinical appropriateness.
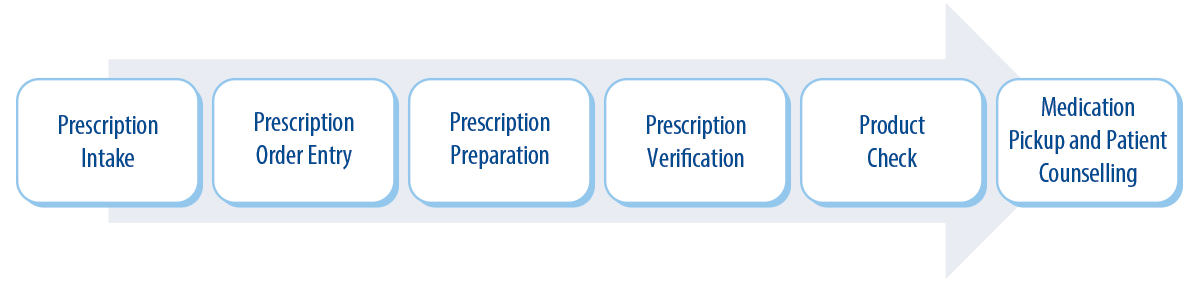
FIGURE 1. Prescription processes described in reports of good catches by community pharmacies.
Figure 2 describes prescription processes (and frequency) at which good catches were made. The good catches were made by the pharmacist or a supporting pharmacy team member in 82% and 15% of the reports, respectively. A small proportion (3%) of the good catches were made by the prescriber before the prescription was dispensed (e.g., through communication with a pharmacy team member) or by the patient or their caregiver at pick up. The most frequently reported type of error prevented was incorrect dose/frequency, which accounted for 20% of all reports (Figure 3).
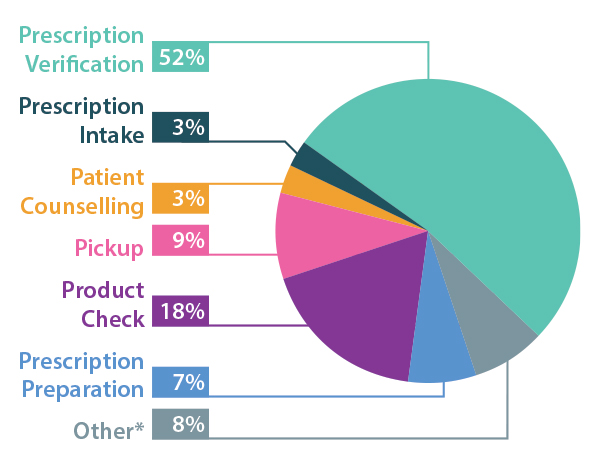
FIGURE 2. Prescription processes at which good catches were made. *”Other” includes medication administration in the pharmacy and other processes.
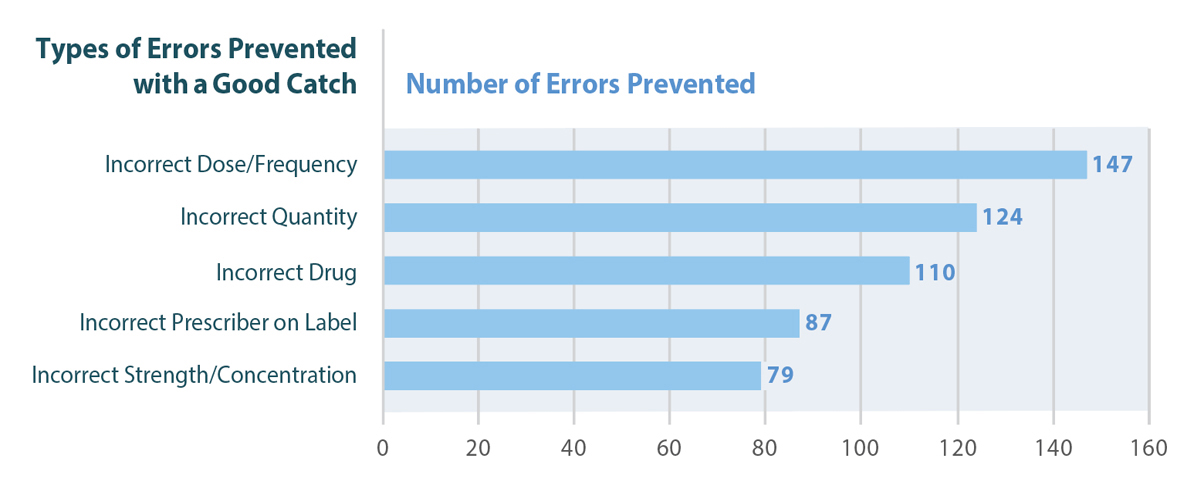
FIGURE 3. Top 5 types of errors prevented with a good catch.
QUALITATIVE ANALYSIS
Three main themes were identified from this data set, each with multiple subthemes (Figure 4). Each theme represents a positive mechanism that permitted the good catch to be made and prevented the incident from reaching the patient.

FIGURE 4. Main themes and subthemes.
THEME: Well-Informed Patients and/or Care Partners
Medication Knowledge and Clear Communication with Pharmacists
Although very few of the reported near-miss incidents were discovered by patients or caregivers, this scenario represents an important opportunity for continuous quality improvement. Patients who were knowledgeable about their medications (e.g., name, indication, dose) were well positioned to detect errors during dialogue with a pharmacist. Similar findings were captured in a multi-incident analysis of consumer-reported incidents.6
Incident Example: During counselling about ciprofloxacin ear drops, a patient informed the pharmacist that the prescription was for an eye infection. The pharmacist consulted the prescriber, and the order was changed to ciprofloxacin eye drops. The correct product, correctly labelled, was then provided to the patient.
THEME: Human Resources
Empowered Pharmacy Support Staff
The good catches in this subtheme resulted from active participation in medication safety practices and error detection by engaged, well-trained members of the pharmacy support team (technicians, assistants, and students). Most errors in this subtheme were detected by pharmacy support staff, in consultation with the patient, reinforcing the value of good communication with well-informed patients and/or care partners.
Incident Example: Prescriptions intended for 2 different patients were mistakenly placed together in the same bag. When one of the patients came to pick up their medications, the pharmacy assistant noticed the error while performing physical verification of the vials before handing them to the patient.
Availability of a Second Pharmacist
In several of the reported incidents a second pharmacist, available to verify prescriptions and products, was able to identify errors overlooked by the pharmacist who initially checked the prescription order entry. While it is recognized that not all pharmacies can be staffed with a second pharmacist, this additional resource and check support medication safety.
THEME: Pharmacy Team Member Intervention
Within the pharmacy processes, there are multiple points where a pharmacy team member can help to catch errors before they reach the patient.8 Each subtheme represents a key opportunity at which errors can be prevented.
During Prescription Verification
Prescription verification encompasses verification of prescription order entry, as well as verification of clinical appropriateness. During clinical verification, the pharmacist assesses the clinical appropriateness of the prescribed medication. This includes checking dosage and directions for use of the product and the appropriateness of the product for the patient’s indication, as well as assessing potential drug-drug or drug-disease interactions. Examples of “good catches” at the prescription verification step are described in Box 1.
BOX 1. Examples of good catches during prescription verification.
- A prescription was received for raltegravir potassium 600 mg. This medication, which is used to treat HIV infections, is only available as 400 mg tablets. The pharmacist called the prescriber to clarify the dose and schedule and to confirm the indication for the prescription. It turned out that the physician intended to order potassium chloride 600 mg. The order was changed to potassium chloride.
- Amlodipine was ordered for a patient; however, a pharmacy staff member noted that this medication had been discontinued 6 months earlier. The pharmacist consulted the prescriber and learned that the order had been written in error.
- The pharmacy received a prescription for an antibiotic to treat a patient with a urinary tract infection. The patient had a known allergy to the medication. The prescriber was consulted, and the order was changed to an alternative medication.
- The pharmacy received a faxed prescription for isoniazid 600 mg for the treatment of latent tuberculosis. The pharmacy staff member noted that this was the usual dosage for rifampin, not isoniazid. After discussion with the prescriber, the initial order was cancelled, and a new faxed prescription was received for rifampin 600 mg daily.
- For a patient with a chest infection, the pharmacy received prescriptions for mometasone nasal spray, budesonide/formoterol inhaler, amoxicillin, prednisone, and guanfacine XR. Questioning the use of guanfacine for this patient, the pharmacist contacted the prescriber, who confirmed that the intention had been to prescribe guaifenesin, not guanfacine XR.
- A prescription for levofloxacin 750 mg once daily for 10 days was incorrectly entered as levetiracetam 250 mg, 3 tablets once daily for 10 days. The pharmacist noticed the error during clinical verification.
During Product Check
Many errors were intercepted during the product check step, when the pharmacist or pharmacy technician was verifying the prepared product. This is often the final check in the workflow before the product is packaged (bagged) and set aside for pickup. Examples of processes reported to support the good catches were 1) consistent checks of drug identification numbers (DINs) for compliance packages, 2) standardized communication processes, and 3) efforts to raise awareness of look-alike, sound-alike medications.
During Medication Pickup and Patient Counselling
Within this subtheme, the pharmacy team frequently identified and resolved errors during verification of patients’ identity and patient counselling.
CONCLUSION
This multi-incident analysis of near misses in community pharmacies highlights key areas where effective interventions, or “good catches”, occurred. Pharmacy team members have an important role in patient safety, and near-miss reporting provides valuable insights into this role. The shared learning that results can inform continuous system improvements.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.