Multi-Incident Analysis of Incidents Involving Paramedicine
Often referred to as emergency medical services (EMS) personnel, paramedics provide a critical link in the care of patients in the community for emergency situations and during transport (until patient transfer to receiving facilities). A multi-incident analysis was conducted to identify themes relating to medication errors in paramedicine practice and to highlight opportunities for improvement.

INTRODUCTION
Paramedicine encompasses the provision of prehospital and out-of-hospital emergency, urgent, and preventive medical care. As such, it may include assessment, treatment, and transport (e.g., by ground ambulance or by air medical services) of patients.1 Often referred to as emergency medical services (EMS) personnel, paramedics provide a critical link in the care of patients in the community for emergency situations and during transport (until patient transfer to receiving facilities). A multi-incident analysis was conducted to identify themes relating to medication errors in paramedicine practice and to highlight opportunities for improvement.
METHODOLOGY
Reports of medication incidents related to paramedicine were extracted from reports* submitted to 3 ISMP Canada reporting databases (Individual Practitioner Reporting, Community Pharmacy Incident Reporting, and Consumer Reporting) and the National System for Incident Reporting† (NSIR), from database inception to November 13, 2018. The search was conducted using the keywords “ambulance”, “crew”, “EMT” [Emergency Medical Technician], “EMS”, “paramedic”, and “responder”. Of the 163 reported medication incidents extracted and reviewed for relevance, about one-third were retained for analysis. The analysis was conducted according to the methodology outlined in the Canadian Incident Analysis Framework.2
QUANTITATIVE FINDINGS
Patient harm was reported in 23% of the incidents reported to the ISMP Canada databases and 22% of incidents reported to the NSIR database. About half of all incidents included in the analysis were reported to have occurred during the administration stage of the medication-use process. For reports from the ISMP Canada databases, the most common incident types were dose omission and incorrect drug; among incidents from the NSIR database, incorrect rate/frequency and dose omission were most common. Many of the incidents involved opioids, particularly fentanyl and morphine.
QUALITATIVE ANALYSIS
The analysis revealed 5 main themes (one of which was further divided into 2 subthemes), loosely following elements of the EMS response process (see Figure 1).
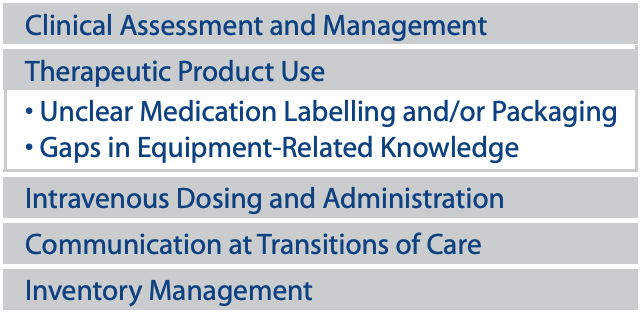
FIGURE 1. Main themes and subthemes
THEME: Clinical Assessment and Management
After paramedics reach the site of an emergency, there is limited time for them to assess the ill or injured patient(s), gather relevant information, and evaluate the clinical concern. The subsequent course of action must be rapidly determined, according to established protocols, guidelines, and treatment options. Given the urgency of certain situations and the lack of access to key data (e.g., test results), information-gathering (e.g., past medical history, medication use) and assessment may be incomplete, which can compromise patient care.
Incident Example
A patient who was experiencing pain called 9-1-1 and self-applied 2 fentanyl patches before EMS arrival and transport. In the ambulance, the patient was given another opioid medication. At the hospital, the patient’s pain appeared to be inadequately controlled, and the physician ordered yet another opioid. The patient was later found unresponsive and experiencing respiratory depression. Neither the paramedics nor the hospital staff had asked about prior opioid use, and they were therefore unaware that the patient had previously been using fentanyl regularly, but was now opioid-naïve due to discontinuation of the medication. As such, the 2 fentanyl patches were “left over”, and self-application of these patches, as well as administration of additional opioid medications in the ambulance and at the hospital, occurred at a time when the patient had reduced opioid tolerance.
When caring for any patient, it is important to ascertain the complete medical history, including current medication use and clinical findings, and to communicate these details to other health care practitioners in the patient’s circle of care. However, the ability to gather information can be limited in some situations (e.g., when treating patients who are critically ill or confused). The patient’s home medication list, if available, can be an important source of medication information to assist in the communication of key findings.3
THEME: Therapeutic Product Use
Subtheme: Unclear Medication Labelling and/or Packaging
Several incident reports identified problems related to the labelling and/or packaging of medications, such as look-alike packaging and ambiguous presentation of expiry dates on labels. The cramped, often poorly lit environment of an EMS vehicle (typically an ambulance), the time pressures of emergency situations, and multiple competing priorities, all contribute to the risk of selection errors related to labelling and/or packaging.3
Incident Example
During a resuscitation attempt on scene, the paramedic mistakenly selected and injected morphine instead of epinephrine.
For purposes of stocking an EMS vehicle, it is important to choose products with easy-to-read labelling and packaging (e.g., prefilled, labelled syringes instead of ampoules). The practice of removing individual vials and ampoules from their outer packages for storage in the EMS vehicle improves access to medications in emergency situations but can also contribute to selection errors.3
Subtheme: Gaps in Equipment-Related Knowledge
Paramedics are trained to use a diverse range of medical devices, equipment, and supplies to care for patients. However, it can be challenging for them to become familiar with and knowledgeable about all of the various products that they may come across, such as a patient’s own device or equipment that is infrequently encountered.
Incident Example
The paramedic crew mistakenly connected a patient’s oxygen tube to the air outlet instead of the oxygen tank, which resulted in a dangerous reduction in the patient’s oxygen saturation.
THEME: Intravenous Dosing and Administration
To initiate and administer intravenous medications in emergency situations, paramedics must carry out several tasks, including inserting the venous catheter, performing dose calculations, and setting up and programming the pump. The analysis identified several factors contributing to the risk of error when performing these tasks, including complex medication dosing regimens, complicated pump adjustments for different medication concentrations and flow rates, and a lack of adequate and visible labelling to identify different medication access lines.
Incident Example
A medication intended for intravenous administration was inadvertently administered into the patient’s arterial line. Fortunately, the patient experienced no harm. The arterial line was later labelled to help in distinguishing it from the intravenous line used to administer medications.
THEME: Communication at Transitions of Care
Paramedics are considered part of a patient’s care continuum, whether as a first responder to an emergency or when transporting the patient to a care facility. In this role, paramedics often act as intermediaries between patients and care facilities or between practitioners in different care settings. Several reports highlighted medication errors resulting from incomplete care transitions between paramedics and other health care practitioners.
Incident Example
A patient was brought to hospital by ambulance. During a verbal hand-off to hospital personnel, the paramedic staff said that the patient had no allergies. In the hospital, a penicillin-related antibiotic was administered to the patient. Later, when hospital staff read the patient’s paperwork, they realized that the patient was allergic to penicillin. Fortunately, the patient did not experience an adverse reaction to the antibiotic.
In the multi-incident analysis, delayed documentation was also implicated in dose-omission errors, as well as in delayed administration of life-saving medications. Although verbal information about the patient’s status is routinely shared during care transition, a complete written account of the care provided in the EMS vehicle is often deferred. This delay and the consequent interim absence of information can affect patient care. A standardized checklist for verbal hand-offs, that includes the need for timely written documentation, may be a helpful approach.
THEME: Inventory Management
Regular review of the inventory maintained within the EMS vehicle, as well as timely and appropriate restocking of medical supplies and medication, are essential. It is important that each piece of equipment and every medication be placed in its correct location and that any partially used or expired products be discarded safely. Design for inventory management and storage should include human factors considerations.4
Incident Example
Nonclinical staff discovered a syringe containing morphine in a medical kit from a previous call for service.
The management of equipment and medication systems should include policies to prevent needlestick injuries, inadvertent exposure to medications, drug diversion, and delays in administering critical care medications to patients. In addition, routine checks of existing stock in EMS vehicles for expired/partially used medications and smart inventory monitoring systems that detect when stock is low and automatically reorder, ensures providers have pertinent life-saving medication on-hand.
CONCLUSION
Medication incidents reported within the EMS/paramedicine context reflect the dynamic and challenging environments in which EMS personnel work. Findings from this analysis form part of the body of evidence that is being used to support local quality improvement initiatives for paramedicine providers. Paramedics are encouraged to report (https://www.ismp-canada.org/err_ipr.htm) medication errors in an effort to support learning and system improvement and to add to the needed body of published evidence on medication management in paramedicine.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.