Newer Classes of Medications for Diabetes Treatment: A Multi-Incident Analysis of Reports from the Community Pharmacy Setting
This bulletin is focused on an analysis of community pharmacy incidents involving newer classes of medications for diabetes treatment, and offers strategies to prevent errors.

INTRODUCTION
Diabetes management is complex, necessitating monitoring and frequent medication changes to achieve optimal glycemic targets. Medications for diabetes treatment are estimated to comprise the fifth most commonly prescribed therapeutic class.1 The newer agents for diabetes also account for several top classes of medications in terms of spending.2 Safety efforts related to diabetes treatment have focused on insulin and older antihyperglycemic agents; errors related to the newer classes of oral and subcutaneous injectable agents are now being reported.3 This bulletin is focused on an analysis of community pharmacy incidents involving newer classes of medications for diabetes treatment, and offers strategies to prevent errors.
METHODOLOGY
Reports of incidents with newer classes of antihyperglycemic medications (also known as antidiabetic medications) (Table 1) occurring in the community pharmacy setting were extracted from 3 ISMP Canada reporting databases (Individual Practitioner Reporting, National Incident Data Repository for Community Pharmacies, and Consumer Reporting) for the period from November 1, 2019, to October 31, 2022. Search criteria included all generic and brand names for the 3 classes of antidiabetic medications available in Canada to extract potentially relevant data.
Reports were excluded from analysis if the incident descriptions were unclear or nonspecific to these classes (e.g., involving errors inputting the incorrect number of refills). The expansion of indications beyond diabetes, for some of the newer medications, has increased the complexity of medication management; there is evidence that some of these medications are being used off-label for weight management. To focus the scope on diabetes treatment, incidents related to Saxenda (liraglutide), which is indicated only for weight loss, and Ozempic (semaglutide), when used off-label for weight loss, were excluded. The analysis was conducted according to the multi-incident analysis methodology outlined in the Canadian Incident Analysis Framework.4
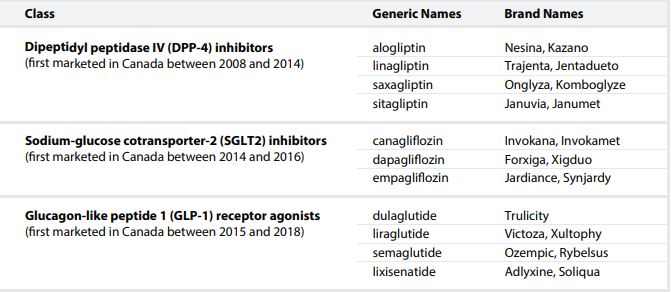
TABLE 1. Generic and Brand Names of the 3 Newer Classes of Antidiabetic Medications Included in the Analysis*
QUANTITATIVE FINDINGS
A total of 770 reports were extracted and screened against the exclusion criteria, with 441 incidents included in the final analysis. Figure 1 highlights the antidiabetic products most commonly reported to be involved in these incidents. The majority of incidents were reported as near misses or as having resulted in no harm; only a small proportion (3.6%) were reported as having caused harm to the patient.
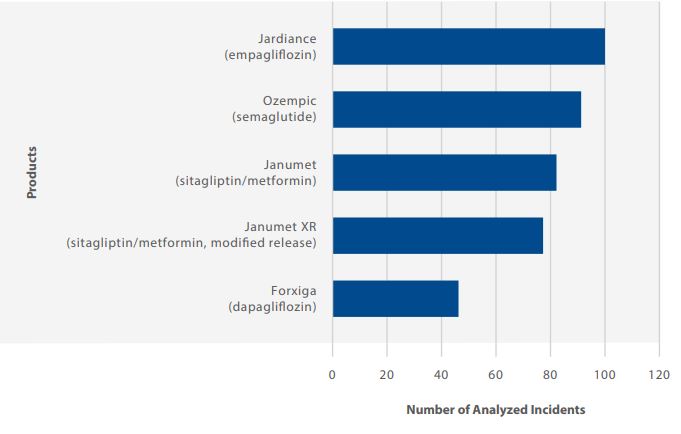
FIGURE 1. Newer antidiabetic products most commonly reported in analyzed incidents.
QUALITATIVE ANALYSIS
The multi-incident analysis identified 3 themes and several subthemes, as summarized in Figure 2 and discussed below.
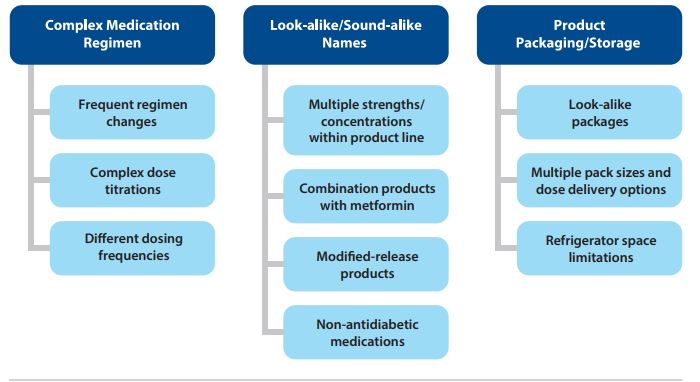
FIGURE 2. Themes and subthemes identified in the qualitative analysis.
THEME: Complex Medication Regimen
Frequent Regimen Changes
Diabetes management often requires adjustments in a patient’s medication regimen. Changes may include dose modifications, addition of an agent from a different medication class, or a switch in medications. A common contributing factor in incidents involving changes to a medication regimen is the copy-over practice, whereby an existing prescription file from the pharmacy system is copied to create an entry for a new prescription.5,6
Complex Dose Titrations
Many medications require dose titration. As one example, for the glucagon-like peptide 1 (GLP-1) receptor agonist class (e.g., semaglutide), titration regimens may be required for a period of weeks and may involve different product strengths; as such, the team must be knowledgeable about the various products available and how to use them.
Incident Example: A patient brought in a new prescription for a titrating dose of semaglutide, to be filled at a later date (i.e., the prescription was to be placed on hold for the time being). Only the first part of the titration regimen was entered into the pharmacy system because pharmacy staff did not recognize that the titration would involve multiple steps and various products. Fortunately, this error was later identified and corrected.
Recent reports of incidents described patients mistakenly administering a starting dose (e.g., semaglutide 0.25 mg weekly) instead of continuing semaglutide 0.5 mg weekly following the prescription refill because the refill label continued to include instructions for the initial starting dose.
Different Dosing Frequencies
Lack of knowledge about differences in dosing frequencies (twice daily vs. once daily) between immediate-release and modified-release formulations (e.g., Janumet and Janumet XR) was frequently described as a factor contributing to incidents. Additionally, lack of awareness of the range of dosing regimens among injectable medications in the GLP-1 receptor agonist class (e.g., once-weekly administration of semaglutide7 and daily administration of liraglutide8 ) was also reported as contributing to the medication errors.
THEME: Look-alike/Sound-alike Names
Many incident reports identified look-alike/soundalike names that affected the prescribing, order entry, and preparation stages. Confusion was reported in relation to the availability of multiple strengths and/or concentrations (e.g., empagliflozin [Jardiance] as 10 mg and 25 mg doses), combination products (sitagliptin alone [Januvia] vs. sitagliptin/metformin [Janumet]), and modified formulations (e.g., Janumet and Janumet XR), in addition to confusion with non-antidiabetic medications (e.g., Synjardy [empagliflozin/metformin] and Synthroid [levothyroxine]).
The following contributing factors, among others, were identified:
- The look-alike nature and use of brand names (e.g., Janumet, Januvia, and Jardiance) in prescriptions without inclusion of generic names.
- The look-alike nature of generic names (e.g., canagliflozin, dapagliflozin, and empagliflozin) without inclusion of brand names.
- Similarities in the display of medications with look-alike names in prescribing and pharmacy order entry systems
THEME: Product Packaging/Storage
Look-alike Packages
One-third of the analyzed reports identified similar packaging as contributing to medication errors. Figure 3 shows images of product pairs that were involved in some of the incidents analyzed.

FIGURE 3. Examples of look-alike packaging described in incident reports.
Multiple Pack Sizes and Dose Delivery Options
Pharmacy teams may not be aware that certain products are available in different pack sizes, with capability of delivering different doses, which may lead to the dispensing of incorrect quantities. For example, liraglutide (Victoza) is available as a multidose pen capable of delivering 3 different doses (0.6 mg, 1.2 mg, or 1.8 mg), and the pens are packaged in 3 different pack sizes (1 pen, 2 pens, or 3 pens). A single pen can deliver 30 doses of 0.6 mg or 10 doses of 1.8 mg. As another example, semaglutide (Ozempic) is available as three different pens: a 2 mg pen that delivers 0.25 mg and 0.5 mg doses; a 4 mg pen that delivers 1 mg doses; and an 8 mg pen (approved, but currently not marketed in Canada) that delivers 2 mg doses.
Incident Example: A prescription for liraglutide (Victoza) 1.2 mg once daily for 90 days was filled with 1 box of 3 pens. Each pen delivers 15 doses of 1.2 mg; therefore, for the specified treatment duration, 6 pens (2 boxes) were required. The pharmacist corrected the quantity before dispensing it to the patient.
Refrigerator Space Limitations
Newer antidiabetic medications for injection (e.g., semaglutide [Ozempic], liraglutide [Victoza], and dulaglutide [Trulicity]) are stored in the refrigerator before the package is opened and also after a prescription is filled (but before it is provided to the patient). Selecting the wrong patient’s filled prescription from the refrigerator was a commonly reported error. These reports highlighted the need to assess and better organize refrigerator space for filled prescriptions to avoid selection errors.
CONCLUSION
This thematic analysis highlights errors related to DPP-4 inhibitors, SGLT2 inhibitors, and GLP-1 receptor agonists occurring in the community pharmacy setting and shares selected safety tips. Key considerations include modifying pharmacy software display for look-alike product names, implementing barcode scanning technology in pharmacy processes, organizing refrigerator space to ensure separation and visibility of products and individual prescriptions, and reviewing label instructions with patients at prescription pick-up to ensure the information matches what the patient expects to receive. Community-based teams, including prescribers, nurses, pharmacists, and pharmacy technicians, are encouraged to review their own incidents, in addition to the learning from this analysis, to guide improvements to their medication-use process.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.