Fatal Outcome with Sodium Phosphate Enemas
ISMP Canada received a report describing the death of an individual who experienced severe electrolyte abnormalities due to an excess of sodium phosphate administered by enema. This bulletin focuses on the technology-related aspects of the incident, highlighting opportunities to review and test the configurations and functions of electronic medication systems to prevent or mitigate harm.
KEY RECOMMENDATIONS
- Evaluate design of order sets when multiple doses are scheduled to be administered close together (e.g., “q1h × 2 doses”) and consider specifying administration times (e.g., “at 1000h and 1100h”) and date(s).
- Develop clinical decision support alerts specifying maximum dose limits for sodium phosphate enemas, to appear during medication ordering, verification, and administration.
- Manage sodium phosphate enema inventory under the control of the pharmacy, with requirements for clinical verification, bar coding, and patient-specific doses.
- Test your electronic medication systems (e.g., computerized prescriber order entry [CPOE] system, pharmacy information system, and electronic medication administration record [eMAR]), using the incident presented in this bulletin, to assess the potential risk of encountering such incidents in your organization.
INTRODUCTION
As part of an ongoing collaboration with a provincial death investigation service, ISMP Canada received a report describing the death of an individual who experienced severe electrolyte abnormalities due to an excess of sodium phosphate administered by enema. Multiple contributing factors were identified in the review of this incident, and learning was shared by the hospital. This bulletin focuses on the technology-related aspects of the incident, highlighting opportunities to review and test the configurations and functions of electronic medication systems, such as computerized prescriber order entry (CPOE) systems, pharmacy information systems, and electronic medication administration records (eMARs), to prevent or mitigate harm.
INCIDENT DESCRIPTION
A hospitalized older adult required bowel preparation for a procedure. The hospital’s CPOE system included several standardized order sets for bowel preparation, one of which was selected and modified by the prescriber to reflect the timing of the procedure. An order similar to the following was entered into the health record:
Sodium phosphate enema q1h
Give 2 enemas; one tomorrow at 1000h and another tomorrow at 1100h
– Start date: [Today]
– Stop date: [Tomorrow]
Of note, the instructions and stop date were adjusted to the next day (i.e., the day of the procedure), but the auto-populated start date (i.e., the day before the procedure) remained unchanged. Additionally, the usual specification in the standardized order set (q1h “for 2 doses”) was inadvertently removed.
The order was verified by a pharmacist for therapeutic appropriateness and was then auto-populated into the eMAR, where it appeared as a scheduled q1h order over 24 hours. The patient received 23 doses, experienced severe electrolyte abnormalities, and subsequently died.
BACKGROUND
Sodium phosphate rectal products are used to treat constipation (at a recommended maximum of 1 enema daily)1 and as bowel preparation before a colonoscopy or other related procedure. For bowel preparation, up to 2 enemas may be given, spaced 30–60 minutes apart, several hours before the procedure.2,3 Sodium phosphate products carry significant risks if used incorrectly. Both Health Canada and the US Food and Drug Administration have issued warnings about potential electrolyte abnormalities and have shared reports of serious effects on the heart and kidney.1,4
CPOE systems with clinical decision support can improve medication safety by guiding users to order medications in a standardized manner consistent with evidence-informed guidelines.5 For clinical decision support to be effective, adequate and up-to-date information must provide prescribers with actionable warnings and timely advice (e.g., embedded maximum dose alerts, potential drug–drug interactions).5 Advanced clinical decision support in the CPOE could also take into account the patient’s renal function, age, and comorbidities to ensure that dosing guidance and maximum dosing limits offered to the prescriber are appropriate for the particular patient.5,6
ANALYSIS FINDINGS
Analysis of the incident identified multiple contributing factors, including the following:
- Auto-population of the start date in the selected standardized order set, which resulted in an earlier start date than intended.
- Absence of alerts in the electronic medication systems (CPOE, pharmacy information system, and eMAR) to communicate to health care providers that the dose, as entered, exceeded the maximum recommended daily dose.
- Supply and storage of sodium phosphate products as stock in the patient care area (i.e., outside of the pharmacy and profiled automated dispensing cabinets [ADCs]), which allowed for use of large quantities without system-based checks.
- Automation complacency (i.e., the monitoring of an automated process less frequently or with less vigilance than optimal because of a low degree of suspicion of error and a strong belief in the accuracy of the technology7), which allowed the incorrect dose to persist throughout the medication-use process.
- Possible knowledge deficits related to appropriate administration of sodium phosphate enemas and risk of harm with overuse.
The analysis also included consideration of practices in other Canadian hospitals to identify additional system vulnerabilities that might exist and to inform recommendations. The following are examples of processes that demonstrate these vulnerabilities:
- Auto-verification of orders for sodium phosphate enemas, without a pharmacist check for appropriate indications, dosing, and drug–drug interactions
- Documentation of the administration of these products in the patient care section of the health record (rather than on the eMAR), without safeguards such as bar coding, maximum dose alerts, drug interaction alerts, and other drug information.
RECOMMENDATIONS
Technology-related recommendations are presented below, some of which were identified by the reporting hospital.
- Remove q1h as a frequency option for bowel preparation order set.
- A bowel preparation order set can incorporate up to 2 doses at specified times to reflect the patient’s needs and timing of the procedure.
- Usability of the order sets and order parameters can be tested with health care providers.
- Create a forcing function in the electronic medication systems (e.g., CPOE, pharmacy information system, and eMAR) that requires a reason for override, to reduce the risk of more than 2 sodium phosphate enemas being ordered, dispensed, and administered to a particular patient within 24 hours.
- Routinely test maximum dose alerts in electronic medication systems, with consideration for alert fatigue.8
- Build easy access to the eMAR from the pharmacy information system to enable a visual check of how the order is displayed in the eMAR, as part of the pharmacist’s order verification process.
- Review the eMAR against the prescriber’s orders to identify discrepancies, as part of the nurse’s order verification process.
- Place sodium phosphate enemas under the control of the pharmacy, requiring clinical verification, bar-coded inventory management, and patient-specific doses (e.g., retrieval from profiled ADCs).
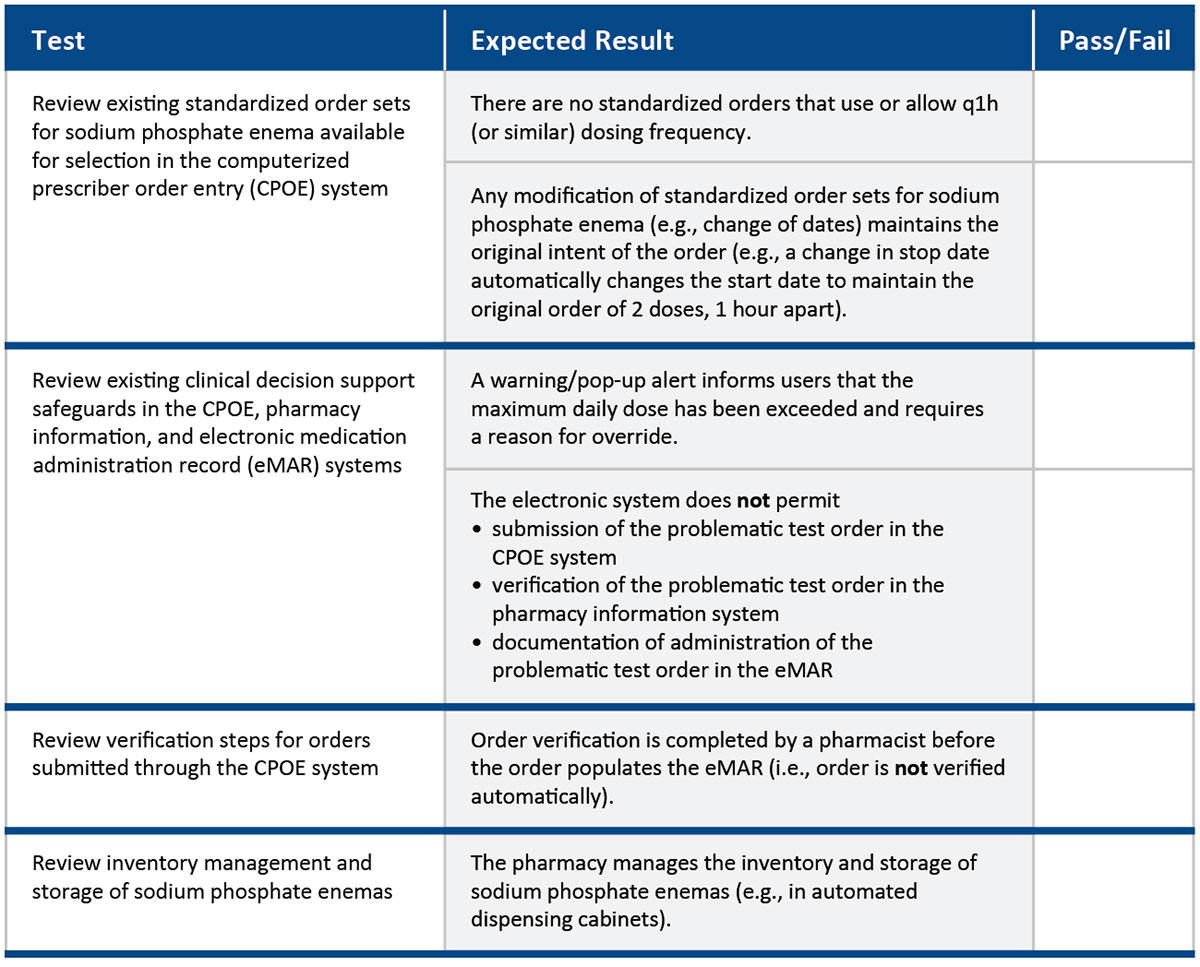
TEST CASE
Test your electronic medication systems using the described incident as a test case to determine whether this error could happen in your organization.
- Open an electronic health record in the CPOE test environment.
- Select a test patient.
- Input “sodium phosphate enema” and review the ordering options.
- Input the medication details from the problematic test order in the incident description above.
- Determine whether safeguards exist, as outlined in the chart below.
- Address any discrepancies identified, and incorporate recommendations from this bulletin.
CONCLUSION
Sodium phosphate administered by enema can cause significant harm when given in excess. Proactive testing of the CPOE, pharmacy information, and eMAR systems for technology-related vulnerabilities can identify gaps and support patient safety. This learning may be applicable to other medications for which several doses may be ordered over a short period of time. Please consider sharing your experience with this test case and related system improvements at info@ismpcanada.ca.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.