Prevent Harm from Midodrine and Midamor Mix-Ups
This bulletin aims to increase awareness of the potential for inadvertent selection errors (e.g., during order entry or when obtained from pharmacy shelves) involving midodrine and Midamor (amiloride), identify factors that contribute to them, and recommend risk reduction strategies to prevent harm.
INTRODUCTION
ISMP Canada has received multiple reports describing outcomes of harm, including death, as a result of inadvertent selection errors involving midodrine and Midamor (amiloride). Incidents involving these two medications have previously been published1,2 and continue to be reported. This bulletin aims to increase awareness of the potential for such mix-ups (e.g., during order entry or when obtained from pharmacy shelves), identify factors that contribute to them, and recommend risk reduction strategies to prevent harm.

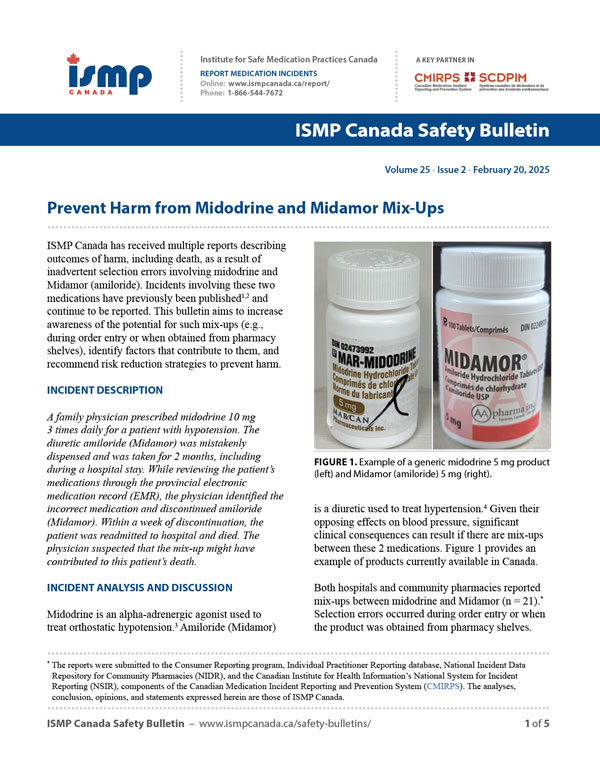
FIGURE 1. Example of a generic midodrine 5 mg product (left) and Midamor (amiloride) 5 mg (right).
INCIDENT DESCRIPTION
A family physician prescribed midodrine 10 mg 3 times daily for a patient with hypotension. The diuretic amiloride (Midamor) was mistakenly dispensed and was taken for 2 months, including during a hospital stay. While reviewing the patient’s medications through the provincial electronic medication record (EMR), the physician identified the incorrect medication and discontinued amiloride (Midamor). Within a week of discontinuation, the patient was readmitted to hospital and died. The physician suspected that the mix-up might have contributed to this patient’s death.
INCIDENT ANALYSIS AND DISCUSSION
Midodrine is an alpha-adrenergic agonist used to treat orthostatic hypotension.3 Amiloride (Midamor) is a diuretic used to treat hypertension.4 Given their opposing effects on blood pressure, significant clinical consequences can result if there are mix-ups between these 2 medications. Figure 1 provides an example of products currently available in Canada.
Both hospitals and community pharmacies reported mix-ups between midodrine and Midamor (n = 21).* Selection errors occurred during order entry or when the product was obtained from pharmacy shelves. Table 1 highlights that more than half of the reports described Midamor (amiloride) being prepared or dispensed when midodrine was intended.
TABLE 1. Mix-ups between midodrine and Midamor (amiloride) captured in incident reports (n = 21).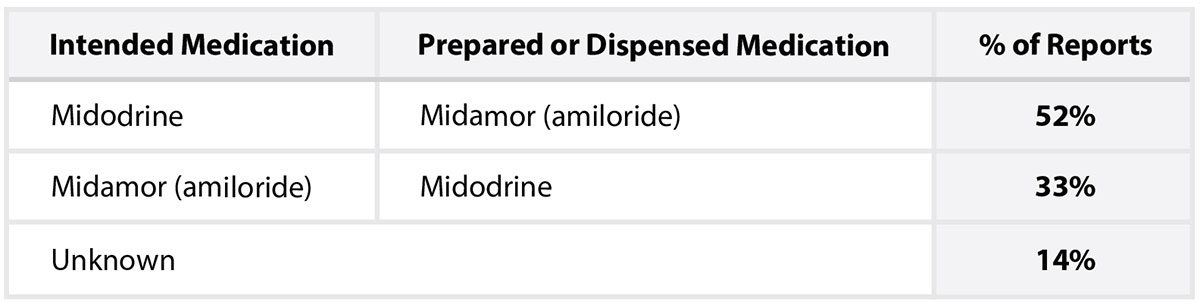
When “mid” is entered into electronic prescribing, pharmacy, or automated dispensing systems, midodrine and Midamor may be displayed adjacently, with overlapping tablet strengths (Figure 2). In the incident described above, the electronic prescription entry correctly specified “midodrine 10 mg TID [3 times daily]”.
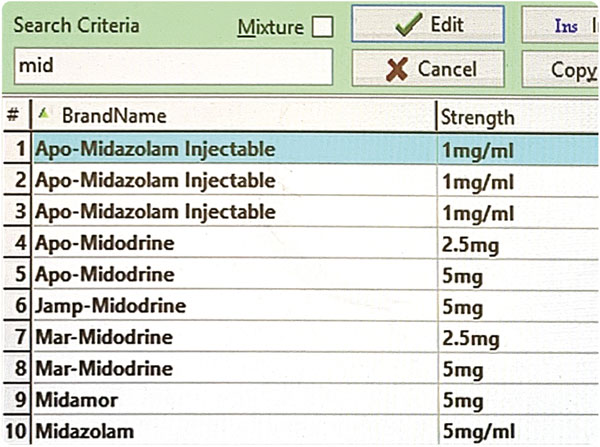
FIGURE 2. Example of a drop-down menu in a community pharmacy computer system.
However, because the e-prescribing and pharmacy systems were not integrated, a separate entry into the pharmacy system was required. During this transcription process, Midamor 5 mg tablet was incorrectly selected from the drop-down menu, and the wrong drug was dispensed to the patient. Instructions on the label directed the patient to take 2 tablets 3 times daily.
During the pharmacist clinical verification step, the incorrectly selected medication and the unusual 3 times daily dosing regimen were not reconciled: notably, midodrine is usually taken 3 to 6 times per day,3 whereas amiloride (Midamor) is typically taken 1 or 2 times per day, depending on the indication.4 The mix-up was not identified when the prescription was refilled 30 days later.
CONTRIBUTING FACTORS
The following sections outline some of the factors that can potentially contribute to mix-ups between midodrine and Midamor, categorized by the stage of the medication-use process where they may originate.
Prescribing
- Lack of indication for medication on the prescription
- Prescribing modules of EMRs that require entry of only 3 letters of a medication name before the drop-down menu options appear for selection
- Limited discussion with patient/caregiver(s) about their understanding of the medication5
Transcribing or Documenting
- Lack of integration between prescribing and pharmacy dispensing softwares, necessitating transcription6
- Pharmacy dispensing software that requires entry of only 3 letters of a medication name before the drop-down menu options appear for selection
- Missed opportunities to ask the patient about the expected medication, dose, and indication during prescription intake

Dispensing
- Missed opportunities for double checks5 of the product against the prescription
- Missed opportunities for double checks5 of product selection (e.g., drug identification number checks, bar code technology)
- Prominence of the brand name on the Midamor product label
- Similar labelling and packaging5 (i.e., when midodrine and Midamor were procured from the same manufacturer)
- Storage of midodrine and Midamor stock bottles next to each other5
- Limited familiarity with the medication midodrine, as well as the brand name for amiloride (Midamor)
Administering
- Missed opportunities for discussion with the patient to verify expected medications and their respective indications
- Lack of bar code scanning at the point of administration

Monitoring
- Lack of follow-up5 to assess patients for unexpected adverse effects and/or treatment failure
- Limited familiarity with the opposing effects on blood pressure by midodrine and amiloride (Midamor)
RECOMMENDATIONS
The following recommendations are presented to reduce the risk of mix-ups between midodrine and Midamor; they incorporate related guidance for preventing incidents involving look-alike/sound-alike products.
Leadership in Community Pharmacies and Health Care Organizations
- In electronic software libraries (e.g., drop-down menus), include the generic name, amiloride, wherever the brand name Midamor appears (i.e., “amiloride [Midamor]”).
- Consider including additional information (e.g., warning for potential mix-up, indication for midodrine) in computerized systems, such as prescribing modules, pharmacy dispensing software, and automated dispensing units.7,8 Additional information can also be affixed to packaging9 and/or in storage areas.5
- Work with EMR and pharmacy software vendors to require, at a minimum, 5 letters of the intended medication name to be typed before options are presented in a drop-down menu for selection.10
Health Care Providers
Prescribers
- Include both the brand and generic names of drugs11,12 in electronic and written prescriptions.13
- Include the indication11 on every prescription (e.g., “midodrine for orthostatic hypotension”) to support a pharmacist’s clinical assessment.10,12 An example strategy shared with ISMP Canada described a prescriber adding indication information to their “favourites” within the prescribing module of an EMR.
- Discuss with patients their prescribed medication(s)11 and the intended benefits so they can confirm the expected medication(s) at pickup from the pharmacy5 and can self-monitor for safety and effectiveness.
Pharmacy Teams
- At prescription intake, document in the patient profile the indication for the medication. Use this information to assess the appropriateness of therapy, including when processing refills.
- Design storage areas to differentiate look-alike products (e.g., separate baskets, labelled shelves).5,10
- Incorporate consistent use of bar code technology11 and drug identification number checks in the dispensing process to mitigate selection errors when products are obtained from the shelves.
- During counselling, discuss what medication the patient is expecting, its intended use, and how they can self-monitor for safety and effectiveness. Open the vial and show the medication that has been dispensed.8,14
- Regularly review identified look-alike/sound-alike medication pairs with the pharmacy team and implement risk reduction strategies together.
Pharmaceutical Manufacturer
- Give prominence to the generic name15 (amiloride) on the Midamor product label to minimize risks and prioritize patient safety.†
CONCLUSION
Health care organizations and providers are encouraged to review the potential for mix-ups involving midodrine and Midamor (amiloride) and to take action to prevent harmful outcomes. Many incident reports highlighted good catches when general strategies to prevent look-alike/sound-alike errors had been implemented and/or when the patient or caregiver was engaged in the treatment plan so that incidents could be detected before harm occurred.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.