Palliative Care at Home – PART 1: MULTI-INCIDENT ANALYSIS
Palliative care provides symptom management and supportive care to patients living with serious or life-limiting illness. Increasing numbers of patients choose to receive this form of care in the home. This bulletin, the first of a 2-part series, describes a multi-incident analysis of medication incidents associated with community-based palliative care across Canada.
INTRODUCTION
Palliative care provides symptom management and supportive care to patients living with serious or life-limiting illness.1 Increasing numbers of patients choose to receive this form of care in the home.2 This bulletin, the first of a 2-part series, describes a multi-incident analysis of medication incidents associated with community-based palliative care across Canada. The second bulletin of this series will describe an analysis of a fatal incident involving HYDROmorphone used for pain management in a palliative home care setting. These bulletins share safety recommendations for continuous improvement in the provision of palliative care.

METHODOLOGY
Medication incidents associated with community-based palliative care, submitted in the 5-year period between October 2020 and September 2025, were extracted from ISMP Canada’s National Incident Data Repository for Community Pharmacies (NIDR), Consumer Reporting program, and Individual Practitioner Reporting database.† Search terms included “palliat*”, “end of life”, “DNR”, and “terminal”. Reports were excluded if the incidents occurred in hospitals, long-term care homes, or other settings that were not the home environment. Palliative care in such settings was the focus of a previous multi-incident analysis.3 The current multi-incident analysis was conducted according to the methodology outlined in the Canadian Incident Analysis Framework.4
QUANTITATIVE FINDINGS
Of the 231 incidents that were retrieved,‡ 79 were included in the analysis after applying the exclusion criteria above. The included reports described near misses (28%), as well as incidents with outcomes of no harm (62%) and harm (10%). The most common types of incidents were incorrect dose (41%), incorrect drug (16%), and incorrect quantity (14%). Figure 1 illustrates the top 5 medications reported to be involved, of which 3 are opioids. Figure 2 shows that most incidents were reported to have been discovered by pharmacists (44%) or nurses (32%).
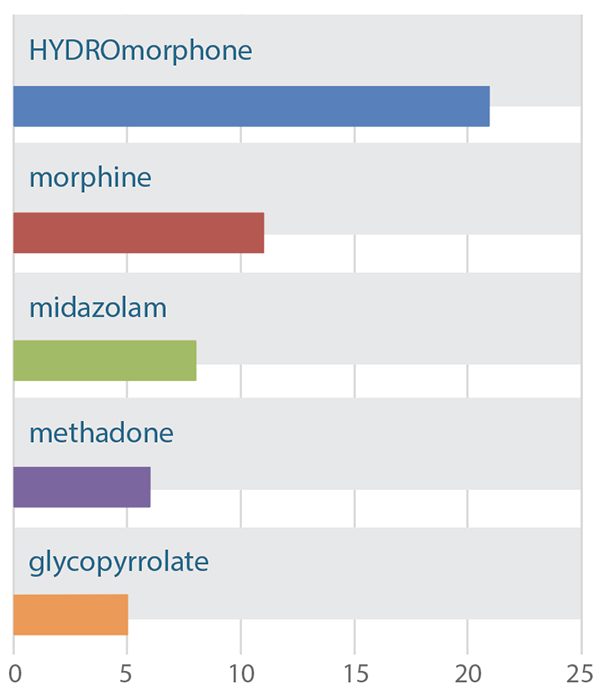
FIGURE 1. Top 5 medications reported to be involved in community-based palliative care incidents.
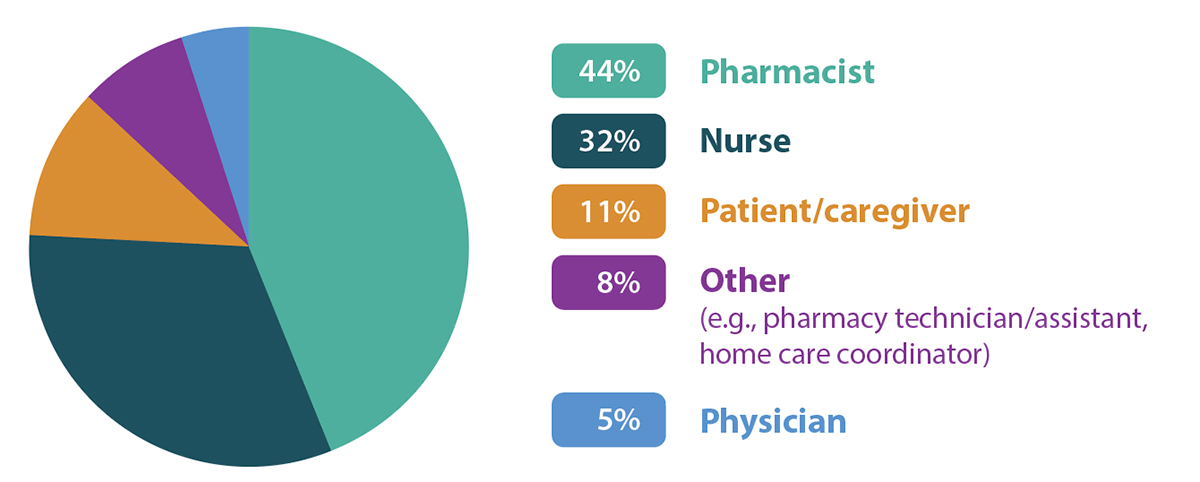
FIGURE 2. Distribution of reported incidents in community-based palliative care, categorized by discoverer.
QUALITATIVE ANALYSIS
The qualitative analysis identified 2 main themes and multiple subthemes related to palliative care in the community setting (Figure 3).
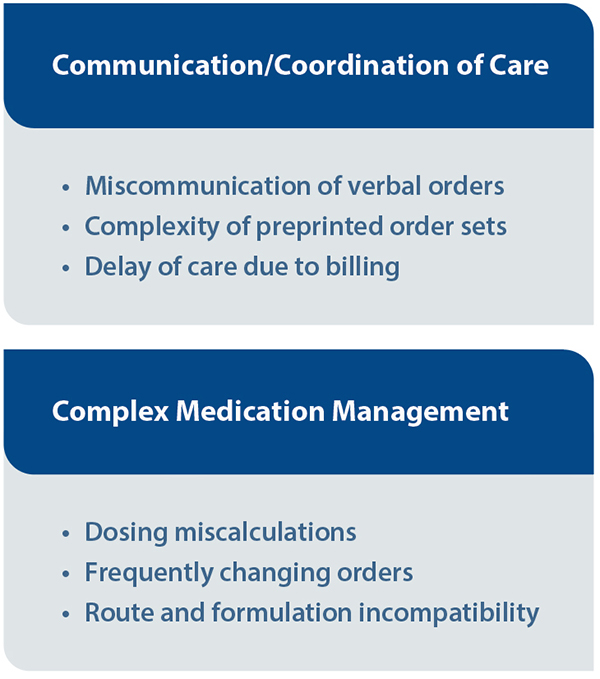
FIGURE 3. The 2 main themes and associated subthemes identified in the analysis.
THEME: Communication/Coordination of Care
Individuals receiving palliative care at home often receive care from multidisciplinary teams that can include prescribers, pharmacists, nurses, and caregivers, with elements of care provided in various locations (e.g., clinic, community pharmacy, home). Some of these health care providers may visit only periodically or may provide only on-call services. As recognized in the previous multi-incident analysis,3 the safe and effective delivery of palliative care depends on clear communication and coordination among all members of the care team.
SUBTHEME: Miscommunication of verbal orders
The current analysis identified several incidents in which verbal (phone) communication between care team members resulted in errors. Some reports also highlighted delays in care related to the lack of a process for timely retrieval of verbal orders from voicemail systems.
Safety tips:
- Limit verbal orders to times when faxing or electronic prescribing are not possible or would create undue delay.
- Use the “read-back” technique to repeat the complete order back to the prescriber as documented, and immediately transcribe or enter the medication order into its permanent record (e.g., patient chart, pharmacy profile).5
- Where applicable, create a procedure for regularly scheduled voicemail checks and ensure the procedure prioritizes time-sensitive medication orders.
SUBTHEME: Complexity of preprinted order sets
Preprinted order sets can set out standardized, evidence-informed medication options and dosing for palliative care, with the aim of improving patient safety. If, however, such order sets become too complex or cumbersome for users to navigate (e.g., poor design, too many choices, distracting information) or are not used as intended, errors may occur.
Incident example: The pharmacy received a patient’s palliative care protocol sheet that included a checkmark next to “morphine” in the order section; this drug was dispensed to the patient. Upon closer examination, however, it was discovered that the checkmark had been crossed off, and a small handwritten note reading “allergy” was documented next to it.
Safety tips:
- Design evidence-informed and end-user-tested palliative order sets to include the essential types of treatment for safe and effective care, organized in a logical layout.
- Include a clearly designated area for additional notes, alerts, and clarifications within the order set so that supplementary information is documented and easy to identify in a consistent location.
SUBTHEME: Delay of care due to billing
Many provinces have specific medication coverage for patients receiving palliative care, subject to various applications and restrictions (e.g., certain medications can only be prescribed by authorized health care providers). Some incident reports described delays in care because of unfamiliarity with the billing processes, including how to determine that a patient’s status was “palliative”.
Safety tips:
- Ensure that preprinted or standardized order sets clearly identify the information needed to facilitate timely prescription processing for palliative medications (e.g., prescriber licence number, patient’s “palliative” status).
- Create a checklist for billing procedures for palliative care treatments that have complicated reimbursement requirements.
THEME: Complex Medication Management
Patients receiving palliative care often require individualized and frequently adjusted medication regimens to meet their changing health care needs.
SUBTHEME: Dosing miscalculations
Several incident reports mentioned incorrect calculations of medication strengths and doses.
Incident example: A patient receiving palliative care had a prescription for methadone 1 mg buccally at bedtime, which noted the quantity to be dispensed as 50 mL of methadone 1 mg/mL. The pharmacy selected methadone 10 mg/mL and mistakenly dispensed 50 mL, with a 3-mL oral syringe to aid administration. The caregiver could not calculate the volume for the 1 mg dose and gave the patient 0.5 mL (using the lowest marking on the syringe). The caregiver called the pharmacy to clarify the volume, and the 5-fold overdose was recognized. The patient experienced excessive drowsiness, and the poison centre representative suggested continued monitoring at home unless symptoms worsened.
Safety tips:
- Incorporate an independent double check, or a delayed self-check,6 against the original prescription (and any relevant calculations) before dispensing or administering high-alert medications.7
- When possible, eliminate the need for bedside calculations by providing formulations that meet the patient’s dosing requirements.
SUBTHEME: Frequently changing orders
Palliative care may require timely changes in medication orders to meet evolving clinical needs.
Safety tips:
- Note on the prescription any intentional changes to a medication, dose, or directions for use (e.g., increased dose, decreased frequency).8
- Ask the patient/caregiver open-ended questions each time a prescription is received, to help determine if there have been changes to the medication regimen.6
- Reconcile the prescribers’ orders, the pharmacy’s prescription labels, the nurse’s medication administration record, and the medications present in the home during transitions of care (e.g., handoff from home care nurse to patient’s family/caregiver).
SUBTHEME: Route and formulation incompatibility
Patients receiving palliative care may be unable to swallow and need administration of medications enterally (e.g., through a feeding tube) or parenterally (e.g., by subcutaneous injection). The routes of administration available for any particular patient will change with their health status, requiring regular reassessment of the suitability of each medication’s formulation.
Incident example: A patient receiving palliative care at home was unable to swallow and was therefore given a new prescription for an orally dissolving tablet. A previous prescription for the same medication, in the form of a regular tablet, was inadvertently copied during order entry, and the formulation was not changed. The home care nurse alerted the pharmacy team, and the correct product was dispensed.
Safety tips:
- Use a pop-up alert in prescribing and dispensing software to add information about a patient’s status with respect to medication administration (e.g., cannot swallow, injectables only).
- Add a clinical alert to the pharmacy profile to inform team members when patients have medication administration limitations. Use this information to assess the compatibility of the medication formulation and route of administration for each prescription received.
- Remove medications from the patient’s home that are no longer appropriate for the route of administration, and clearly communicate the changes to caregivers.
CONCLUSION
This multi-incident analysis identified important considerations related to the communication and coordination of care and complex medication management to meet the needs of patients receiving palliative care. Findings from this analysis highlight opportunities for community care providers to improve the safety of palliative care, which is increasingly provided at home.
Upcoming ISMP Canada Safety Bulletin
Palliative Care at Home
Part 2: Analysis of a Fatal Incident
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.