Palliative Care at Home – PART 2: ANALYSIS OF A FATAL INCIDENT
Palliative care provides symptom management and supportive care to patients living with serious or life-limiting illness. Increasing numbers of patients choose to receive this form of care in the home. This bulletin, the second of a 2-part series, describes the analysis of a fatal incident involving HYDROmorphone used for pain management in a palliative home care setting and shares recommendations for the safe procurement, prescription, administration, and monitoring of opioid medications provided in palliative care kits.
INTRODUCTION
Palliative care provides symptom management and supportive care to patients living with serious or life-limiting illness.1 Increasing numbers of patients choose to receive this form of care in the home.2 The previous bulletin in this 2-part series (Part 1) described a multi-incident analysis of medication incidents associated with community-based palliative care across Canada. This bulletin (Part 2) describes the analysis of a fatal incident involving HYDROmorphone used for pain management in a palliative home care setting and shares recommendations for the safe procurement, prescription, administration, and monitoring of opioid medications provided in palliative care kits (also known as a symptom management/relief/response kits).
INCIDENT DESCRIPTION
A patient receiving palliative care in the home was given an incorrect dose of HYDROmorphone prepared from a symptom management kit. The prescription specified HYDROmorphone 1 mg subcutaneously every 1 hour as needed, but the patient received 4 doses of 10 mg each (i.e., 10 times the prescribed dose)* over a period of about 10 hours. The incorrect dose was eventually recognized, and the patient was transferred to hospital. The patient was treated with naloxone but died several days later due to overdose- and disease-related complications.
BACKGROUND
Symptom Management Kits
Palliative care involves a patient-centred approach that focuses on relieving pain and other distressing symptoms (e.g., nausea, anxiety, shortness of breath) to improve quality of life.4 Symptom management kits (Figure 1) can be used to manage distressing symptoms in the home and minimize emergency department visits and hospitalization.
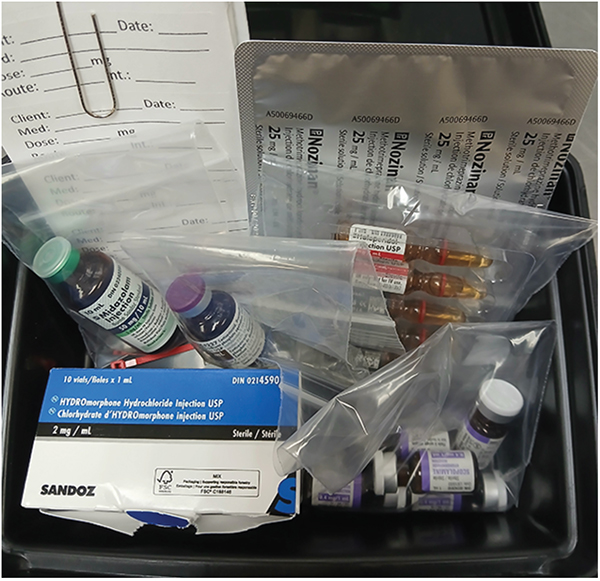
FIGURE 1. An example of a symptom management kit.
Symptom management kits are currently available in multiple provinces. These kits contain preselected medications commonly required for symptom management in palliative care, for example, opioid medications for pain, haloperidol for nausea and agitation, and anticholinergic medications for excess secretions. Typical routes of administration for these medications are non-oral (e.g., injectable, sublingual, rectal). These kits are typically dispensed by a community pharmacy.
Opioid Medications
Opioid medications are high-alert medications5 commonly used in palliative care to manage moderate-to-severe pain and to relieve shortness of breath.6
In the recent multi-incident analysis of incidents associated with palliative care at home, HYDROmorphone and morphine were the medications most often reported to be involved in medication incidents.7 Symptom management kits may include HYDROmorphone (at concentrations of 2 mg/mL and/or 10 mg/mL) or morphine (at concentrations of 2 mg/mL and/or 10 mg/mL and/or 15 mg/mL).
The signs and symptoms of opioid toxicity can include extreme drowsiness, dizziness, confusion, seizure-like movement, pinpoint pupils, and slowed to absent breathing.8
INCIDENT ANALYSIS AND DISCUSSION
Figure 2 summarizes selected key factors contributing to the incident described above, according to the categories described in the Canadian Incident Analysis Framework.9
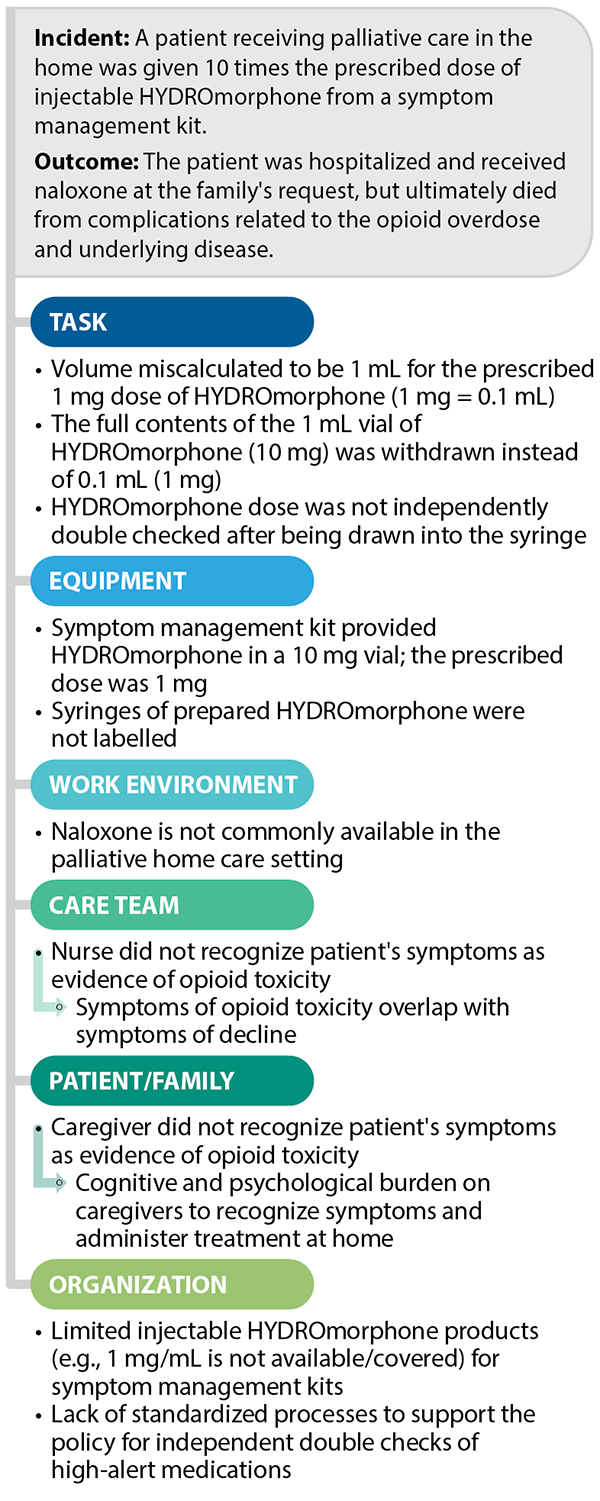
FIGURE 2. Selected factors contributing to a fatal incident involving HYDROmorphone used for pain management in the palliative home care setting.
Analysis of this incident identified several findings that may have contributed to HYDROmorphone overdose.
- Limited available strengths for injectable HYDROmorphone (e.g., 1 mg/mL not available) in symptom management kits increased the likelihood that the patient-specific dose would be prepared incorrectly.
- Provision of a high-concentration HYDROmorphone product for a low dose increased the likelihood that the incorrectly calculated and prepared dose would lead to opioid toxicity.
- Lack of labelling of the prepared syringe containing HYDROmorphone (with labelling limited to a brief note handwritten on tape that was applied to the cup holding the prepared syringe [Figure 3]) decreased the likelihood that a dosing error would be detected.
- Lack of an independent double check of the prepared dose of HYDROmorphone decreased the likelihood that a dose preparation error would be detected before administration, whether by the nurse or another caregiver.
- Lack of standardized processes to support the policy for independent double checks of high-alert medications increased the likelihood that an independent double check would not be performed.
- Knowledge gaps related to the signs and symptoms of opioid toxicity (as compared to signs and symptoms expected with palliative decline)10 decreased the likelihood that the inadvertent opioid overdose would be detected.
- Lack of a standardized protocol for making naloxone kits available in the palliative home care setting decreased the likelihood that an opioid overdose could be treated in a timely manner.
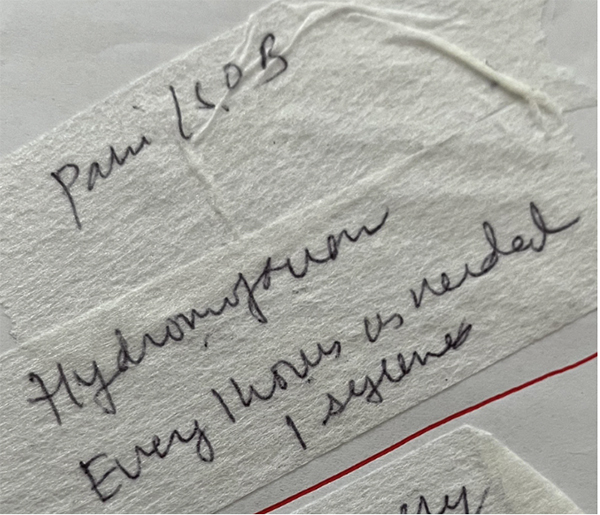
FIGURE 3. Image of the tape label applied to the cup into which the nurse placed the unlabelled syringe of HYDROmorphone for a caregiver to administer to the patient as needed for pain and/or shortness of breath (denoted as “SOB” in the image).
RECOMMENDATIONS
The following system-based recommendations11 for provincial/territorial health care organizations and home health care provider teams incorporate improvements suggested by the patient’s caregivers.
Provincial/Territorial Health Care Organizations
- Review options for the concentrations of injectable opioid products available for symptom management kits (e.g., include HYDROmorphone 1 mg/mL) to allow more patient-specific doses to be available in a ready-to-administer format. This measure would minimize the need for calculations, the need for product manipulation, and the risk of preparation error at the bedside, as well as reducing medication waste.
- Include (in the kit) preprinted syringe labels with fields to satisfy all provincial requirements (which may include the medication name, concentration, dose [in mg and mL], and directions for use).
- Develop a standardized process to support the policy for independent double checks of high-alert medications (e.g., requiring documentation of independent checks after dose preparation).12
- Consider a provincial/organizational policy requiring that naloxone kits (which include an educational pamphlet for the user)13 be paired with symptom management kits, in case of overdose.
- Supporting education for the caregivers at home would include instructions on how to contact the care team before administering naloxone to the patient, even in the case of accidental overdose, to aid the caregivers in making an informed decision.
- Develop a standardized opioid overdose assessment tool to help distinguish between the signs and symptoms of opioid toxicity and the signs and symptoms of natural decline. The tool could include consideration of clinical presentation, onset of symptoms in relation to opioid exposure, and response to opioid dose adjustments.10
Community Pharmacy Teams
- Describe the opioid dose in mg and mL on the prescription label, to minimize the need for volume calculation (by the home care nurse, family member, or other caregiver) at the patient’s bedside.
- Include (in the kit) appropriate syringes for the prescribed dose (e.g., ensure that the desired volume is visible on the syringe’s gradations).
- Counsel the patient’s caregiver (in person or by phone) on the dose to be administered.
- Provide a naloxone kit with symptom management kits, with training for appropriate and safe use.
Home Health Care Provider Teams
- Select the lowest opioid concentration available in the standardized order set for the intended dose, to mitigate the risk of harm from dose preparation errors.
- Prepare medication doses for a caregiver to administer in an appropriate syringe for the prescribed dose and calculated volume (e.g., ensure that the desired volume is visible on the syringe’s gradations).
- Label each prepared syringe in a way that does not obscure the gradations on the syringe.
- Conduct and document an independent double check for all high-alert medications12 prepared in the patient’s home against the order set and pharmacy label.
- If necessary, the double check can be completed by a colleague virtually (using pictures or videos).12
- The double check may be augmented by a tertiary check from a caregiver, especially if they are expected (and trained) to administer the medication when the nurse is not present.
CONCLUSION
This bulletin has identified opportunities to strengthen the safe procurement, prescription, administration, and monitoring of opioid medications provided in symptom management kits for patients receiving palliative care. Expanding product availability, requiring safeguards during medication preparation (i.e., appropriate labelling and independent double checks), and enhancing clinical knowledge to help recognize signs and symptoms of opioid toxicity, can improve medication safety in the palliative home care setting.
![]()
The Canadian Medication Incident Reporting and Prevention System (CMIRPS) is a collaborative pan-Canadian program of Health Canada, the Canadian Institute for Health Information (CIHI), the Institute for Safe Medication Practices Canada (ISMP Canada) and Healthcare Excellence Canada (HEC). The goal of CMIRPS is to reduce and prevent harmful medication incidents in Canada.
Funding support provided by Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
![]()
The Healthcare Insurance Reciprocal of Canada (HIROC) provides support for the bulletin and is a member owned expert provider of professional and general liability coverage and risk management support.
![]()
The Institute for Safe Medication Practices Canada (ISMP Canada) is an independent national not-for-profit organization committed to the advancement of medication safety in all healthcare settings. ISMP Canada’s mandate includes analyzing medication incidents, making recommendations for the prevention of harmful medication incidents, and facilitating quality improvement initiatives.
Report Medication Incidents (Including near misses)
Online: ismpcanada.ca/report/
Phone: 1-866-544-7672
ISMP Canada strives to ensure confidentiality and security of information received, and respects the wishes of the reporter as to the level of detail to be included in publications.
Stay Informed
Subscribe to the ISMP Canada Safety Bulletins and Newsletters.
This bulletin shares information about safe medication practices, is noncommercial, and is therefore exempt from Canadian anti-spam legislation.
Contact Us
Email: cmirps@ismpcanada.ca
Phone: 1-866-544-7672
©2026 Institute for Safe Medication Practices Canada.